
Blog
Why Most People Fail to Quit Smoking: Root Causes Explained

The Reality: Why Most Quit Attempts End in Relapse
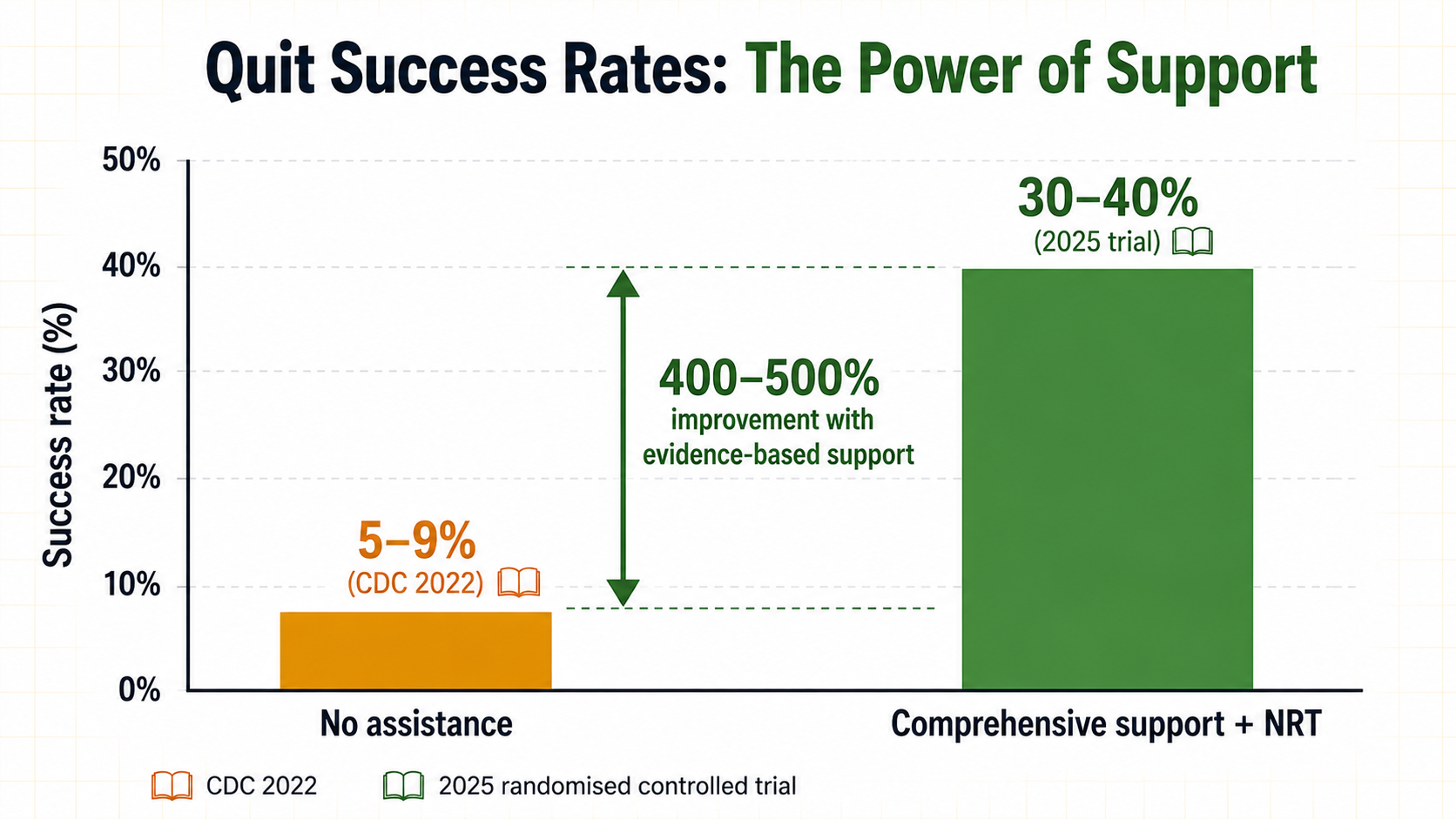
The numbers are stark, yet they tell an important story — not about personal failure, but about the physiological and psychological power of nicotine dependence.
According to CDC data, in 2022, just 9% of smokers who tried to quit were successful on their own [5]. However, a 2025 clinical trial demonstrated that with intensive counseling and appropriate nicotine replacement, success rates rose to nearly 40% [5]. The difference wasn't about grit — it was about addressing the root causes of dependence.
Root Cause 1: Neuroadaptation — Your Brain Has Been Rewired
Nicotine is not a habit. It is a neurochemical hijacker. When you smoke or vape, nicotine reaches the brain within seconds and binds to nicotinic acetylcholine receptors, triggering a flood of dopamine — the "reward" neurotransmitter. Over time, your brain adapts by reducing its natural dopamine production and increasing the number of nicotine receptors. This process is called neuroadaptation, and it makes quitting exponentially harder than simply "deciding to stop."
Root Cause 2: Withdrawal Timeline — The First 72 Hours
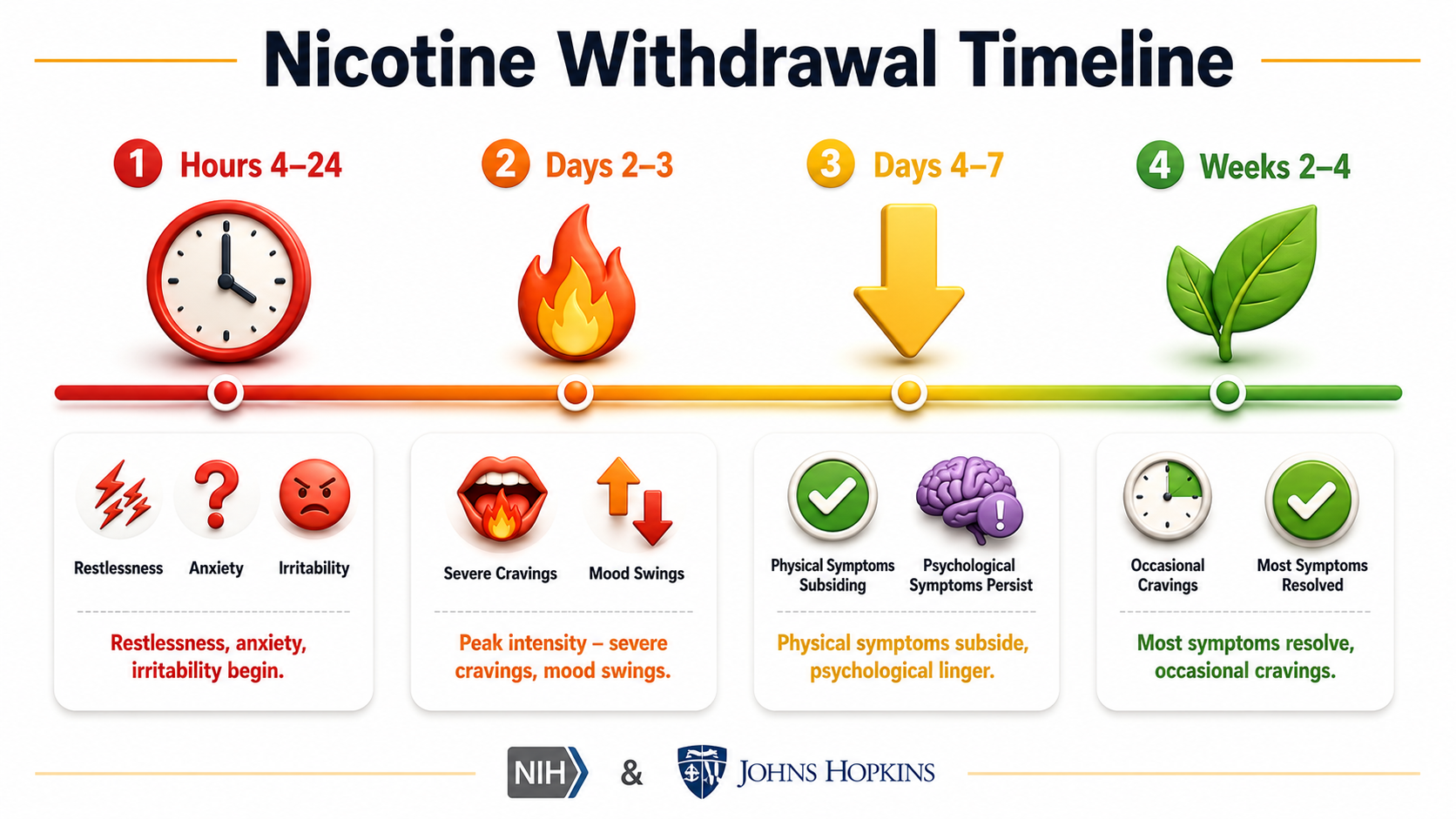
Nicotine withdrawal follows a predictable but brutal timeline. Understanding what happens in your body removes the fear and mystery, making it easier to persevere.
Nicotine levels drop. Symptoms begin: restlessness, anxiety, irritability, difficulty concentrating, and strong cravings. The brain experiences sudden loss of dopamine stimulation [7].
Withdrawal intensity reaches maximum. Physical symptoms include headaches, increased appetite, nausea, constipation. Psychological symptoms: severe irritability, mood swings, anxiety, depression, intense cravings, and sleep disturbances [7].
Physical symptoms begin subsiding significantly. Headaches lessen, sleep improves, energy returns. However, psychological symptoms — irritability, mood changes, cravings — may persist strongly. Many people feel emotionally fragile during this period [7].
Most physical withdrawal symptoms resolve completely. Cravings become less frequent and less intense, though they still occur — particularly in response to triggers (stress, social situations, after meals, coffee). Mood improves, concentration returns to baseline [7].
Critically, withdrawal severity is not a matter of willpower. Genetic factors contribute 50‑75% of the risk for nicotine dependence and also influence withdrawal severity [6]. Some people are simply wired to experience more intense withdrawal — a reality that makes compassionate, evidence‑based support essential.
Root Cause 3: Conditioned Cues — Your Environment Triggers Relapse
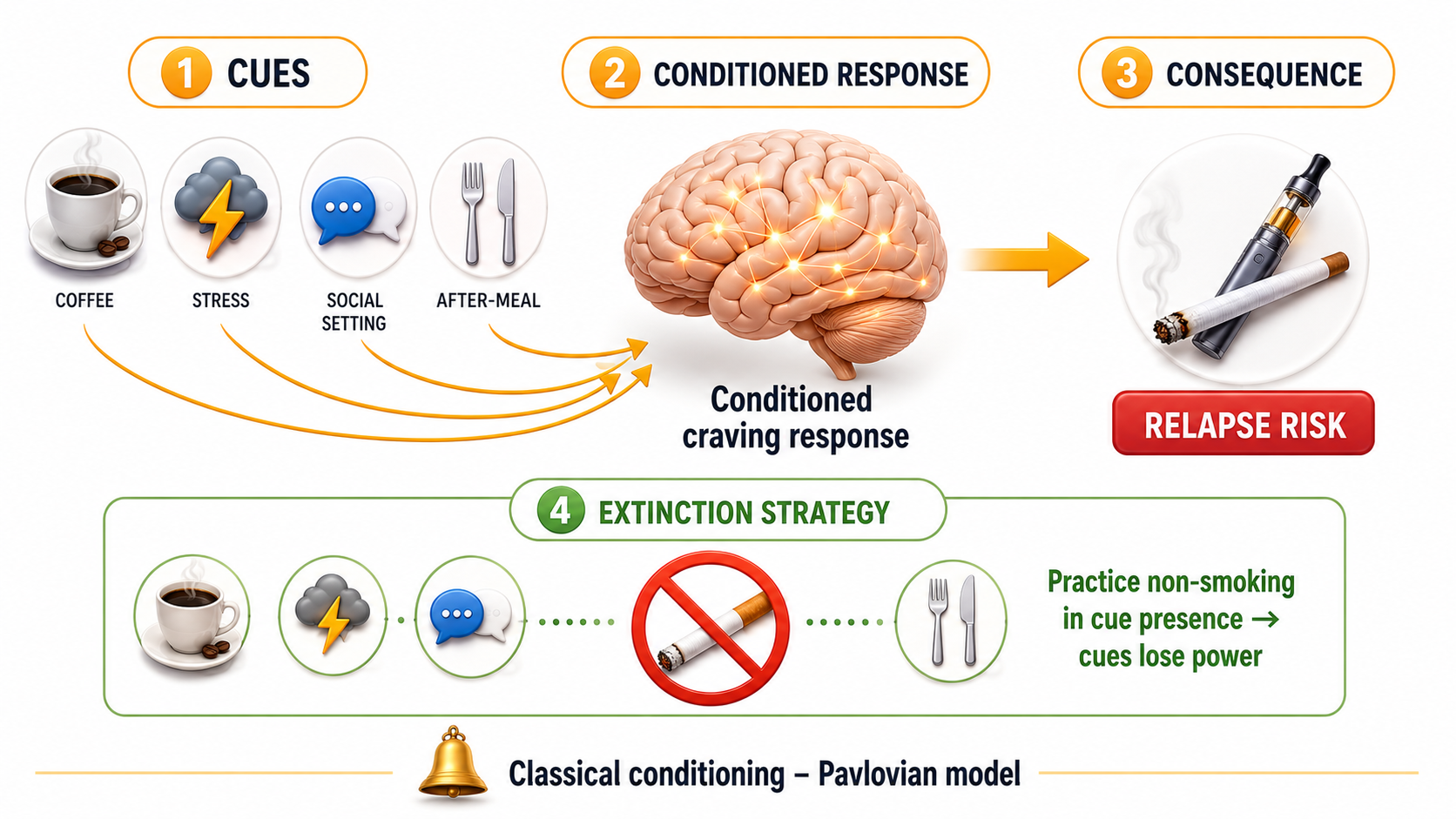
Habits are not just chemical — they are also environmental. Classical conditioning research shows that when a neutral stimulus (a specific location, a time of day, a social situation, or even a smell) is repeatedly paired with nicotine intake, that stimulus becomes a trigger. Over time, simply encountering the cue produces cravings and physiological responses, even without nicotine presence.
In a landmark study, researchers Dr. Lazev and colleagues demonstrated that smokers reported a much greater urge to smoke when they encountered environmental cues paired with smoking than when exposed to cues paired with non‑smoking. Their pulse rates also increased — a measurable physiological reaction — confirming that these conditioned responses are involuntary and automatic [9]. This explains why former smokers often relapse when returning to a familiar bar, after a meal, during a coffee break, or when stressed. The cue itself activates the craving circuit.
Why "Cold Turkey" Fails Most People
Cold turkey — abruptly stopping all nicotine without any aid — has a documented success rate of only 3‑5%. This approach ignores everything known about neuroadaptation and conditioned cues. It's not impossible, but it is the hardest path. The sudden removal of nicotine leaves your brain understimulated (triggering severe withdrawal) and your conditioned cues unaddressed (triggering automatic cravings). Most people who try cold turkey relapse within the first week, often at the 3‑day withdrawal peak, reinforcing the belief that quitting is impossible.
Evidence‑based approaches dramatically improve outcomes. A 2024 meta‑analysis published in Preventive Medicine found that mailout smoking cessation support significantly improved the odds of quitting at six to twelve months (OR = 1.43). Most importantly, interventions that included nicotine replacement therapy were associated with higher odds of quitting (OR = 1.61) compared to behavioral interventions alone (OR = 1.28) [11]. This suggests that for most people, pharmacotherapy support is not optional — it is essential.
The Role of Genetics in Nicotine Dependence
Heritability studies have consistently found that genetic factors account for 50‑75% of the risk for nicotine dependence [6]. This is not a small modifier — it is a major determinant. Specific single nucleotide polymorphisms (SNPs) have been identified that predispose individuals to consume larger amounts of nicotine more frequently and to experience more severe withdrawal symptoms when trying to quit [6]. This genetic vulnerability means that for some people, quitting is objectively harder than for others, regardless of motivation or willpower.
A 2026 meta‑analysis published in Addictive Behaviors examined 4005 participants across nine randomized controlled trials, comparing bupropion combined with nicotine replacement therapy (NRT) versus bupropion alone. The combination therapy significantly improved short‑term abstinence rates (risk ratio = 1.35, 95% CI: 1.22‑1.50, I² = 21%) [10]. This finding suggests that even for those with genetic vulnerability, combined pharmacotherapy can substantially improve outcomes.
Barriers to Access: Why Help Is Often Out of Reach
Even when smokers want help, they often cannot get it. Accessibility to smoking cessation support remains a major barrier. Mailout smoking cessation programs — which deliver support directly to participants' homes — have been shown to be effective, with odds of quitting increased by 43% (OR = 1.43). Interventions delivered for longer than 12 weeks were more effective (OR = 1.57) than shorter programs [11]. This suggests that duration and consistency matter as much as method.
Other barriers include the cost of pharmacotherapy, lack of physician referral, and limited access to specialist cessation counselors. Addressing these structural barriers is as important as understanding the neurobiology of dependence.
A Smarter Path: Reducing Harm Through Complete Switching
For adults who smoke and have tried to quit using conventional methods without success, switching completely to a non‑combustible nicotine product represents a harm reduction strategy. Removing combustion eliminates over 7,000 chemicals found in tobacco smoke, including tar and carbon monoxide. The goal should be complete switching — not dual use — and ultimately, ceasing nicotine use altogether.
However, nicotine itself remains addictive. The same neuroadaptation and withdrawal mechanisms apply to vaping as to smoking. A successful transition is not about replacing one addiction with another but about stepping down nicotine strength over time. Many former smokers start with higher nicotine concentrations (20 mg/mL or more) and gradually reduce to 10 mg/mL, then 5 mg/mL, before stopping entirely.
• Step 1 — Switch completely from cigarettes to a pod system. No dual use — aim for 100% replacement.
• Step 2 — Start at a nicotine strength that matches your previous cigarette consumption.
• Step 3 — Over several months, gradually reduce nicotine strength in small increments.
• Step 4 — Once at the lowest comfortable strength, set a cessation date and stop using nicotine entirely.
• Step 5 — If you relapse, don't give up. Most successful quitters try multiple times before succeeding.
Product Recommendations: Tools for Transition
RELX pod systems are designed for adult smokers transitioning away from combustible tobacco. These devices are draw‑activated, compatible with nicotine salt pods, and require no technical knowledge to operate.
RELX Devices — Simple, Reliable, Effective
RELX Pods — Nicotine Strength Options for Step‑Down
※ Prices are for reference only and may be subject to change. Please check the website for the latest offers. 🔞 Age verification required.
🇦🇺 G'DayVape: We support adult smokers making informed choices about harm reduction. All products are 100% authentic and intended for adult use only. Nicotine is addictive — the healthiest choice is to never use any nicotine product. For those who smoke, switching completely to a non‑combustible product reduces exposure to the most harmful chemicals in tobacco smoke.
📚 References & trusted sources
- Centers for Disease Control and Prevention (CDC) – Current Cigarette Smoking Among Adults in the United States. cdc.gov
- JAMA Internal Medicine – Integrating Tobacco Treatment into Lung Cancer Screening: The Screen Assist Factorial Randomized Clinical Trial (2025). pubmed.ncbi.nlm.nih.gov
- Current Topics in Behavioral Neurosciences (NIH) – Nicotine Withdrawal (2015). pmc.ncbi.nlm.nih.gov [Heritability 50‑75%, SNP influence, withdrawal timeline 4‑24h, peak day 3, taper 3‑4 weeks]
- Johns Hopkins Aramco Healthcare – Nicotine Withdrawal: How to Manage Symptoms and Stay Smoke‑Free. jhah.com [Withdrawal timeline hour‑by‑hour, coping strategies, neurobiology of dopamine]
- Florida Institute of Technology / Lazev et al. (1999) – Classical conditioning of environmental cues to cigarette smoking. fit.edu [Conditioned cues trigger cravings, heart rate increases, conditioned responses are automatic]
- Preventive Medicine (2024) – Evaluating the effectiveness of mailout smoking cessation support: a systematic review and meta‑analysis. pubmed.ncbi.nlm.nih.gov [OR 1.43, NRT superior to behavioral support alone, longer interventions >12 weeks more effective]
- Addictive Behaviors (2026) – Efficacy of combined nicotine replacement therapy (NRT) and bupropion compared to bupropion alone: a systematic review and meta‑analysis. sciencedirect.com [RR 1.35 for short‑term abstinence, 4005 participants, 9 RCTs]
© 2026 G'DayVape — adult vaping knowledge, grounded in clarity. Always adult‑only.
 RELX Pod
RELX Pod